
Laser radiation predominantly causes injury via thermal effects. Even moderately powered lasers can cause injury to the eye. High power lasers can also burn the skin. Some lasers are so powerful that even the diffuse reflection from a surface can be hazardous to the eye.
The coherence, the low divergence angle of laser light and the focusing mechanism of the eye means that laser light can be concentrated into an extremely small spot on the retina. A transient increase of only 10 °C can destroy retinal photoreceptor cells. If the laser is sufficiently powerful, permanent damage can occur within a fraction of a second, literally faster than the blink of an eye. Sufficiently powerful in the visible to near infrared laser radiation (400-1400 nm) will penetrate the eyeball and may cause heating of the retina, whereas exposure to laser radiation with wavelengths less than 400 nm and greater than 1400 nm are largely absorbed by the cornea and lens, leading to the development of cataracts or burn injuries.
Infrared lasers are particularly hazardous, since the body's protective "blink reflex" response is triggered only by visible light. For example, some people exposed to high power Nd:YAG laser emitting invisible 1064 nm radiation, may not feel pain or notice immediate damage to their eyesight. A pop or click noise emanating from the eyeball may be the only indication that retinal damage has occurred i.e. the retina was heated to over 100 °C resulting in localized explosive boiling accompanied by the immediate creation of a permanent blind spot.
Damage mechanisms
Lasers can cause damage in biological tissues, both to the eye and to the skin, due to several mechanisms. Thermal damage, or burn, occurs when tissues are heated to the point where denaturation of proteins occurs. Another mechanism is photochemical damage, where light triggers chemical reactions in tissue. Photochemical damage occurs mostly with short-wavelength (blue) and ultra-violet light and can be accumulated over the course of hours. Laser pulses shorter than about 1 μs can cause a rapid rise in temperature, resulting in explosive boiling of water. The shock wave from the explosion can subsequently cause damage relatively far away from the point of impact. Ultrashort pulses can also exhibit self-focusing in the transparent parts of the eye, leading to an increase of the damage potential compared to longer pulses with the same energy.
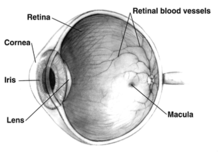
The eye focuses visible and near-infrared light onto the retina. A laser beam can be focused to an intensity on the retina which may be up to 200,000 times higher than at the point where the laser beam enters the eye. Most of the light is absorbed by melanin pigments in the pigment epithelium just behind the photoreceptors, and causes burns in the retina. Ultraviolet light with wavelengths shorter than 400 nm tends to be absorbed in the cornea and lens, where it can produce injuries at relatively low powers due to photochemical damage. Infrared light mainly causes thermal damage to the retina at near-infrared wavelengths and to more frontal parts of the eye at longer wavelengths. The table below summarizes the various medical conditions caused by lasers at different wavelengths, not including injuries due to pulsed lasers.
| Wavelength range | Pathological effect |
|---|---|
| 180–315 nm (UV-B, UV-C) | photokeratitis (inflammation of the cornea, equivalent to sunburn) |
| 315–400 nm (UV-A) | photochemical cataract (clouding of the eye lens) |
| 400–780 nm (visible) | photochemical damage to the retina, retinal burn |
| 780–1400 nm (near-IR) | cataract, retinal burn |
| 1.4–3.0μm (IR) | aqueous flare (protein in the aqueous humour), cataract, corneal burn |
| 3.0 μm–1 mm | corneal burn |
The skin is usually much less sensitive to laser light than the eye, but excessive exposure to ultraviolet light from any source (laser or non-laser) can cause short- and long-term effects similar to sunburn, while visible and infrared wavelengths are mainly harmful due to thermal damage.